After a detailed history & physical examination, few basic laboratory investigations & a sonological evaluation is very important to choose the modality of treatment for infertility as it affects the success rate of the treatment.
We, here at SFWH follow a basic protocol before commencing any treatment of infertility. History taking can be converted into a counselling session which works to break the ice between the couple & doctor. The initial shyness & awkwardness to talk on intimate issue is also lost. Trust & confidence develops which helps the couple to understand & participate in the treatment.
Points to be highlighted in history are duration of infertility, menstrual history, coital frequency, past medical & surgical history, occupational history & history of allergy.
We start the clinical examination of female by measuring her weight & height & then calculating her BMI. Our experience has shown that ladies who have normal BMI not only respond well to the treatment of infertility but also have a better outcome of pregnancy as compared to their obese or underweight counterparts.
After recording the weight, the lady should be escorted into a comfortable examination room by a trained nursing staff where detailed general & systemic examination is done. Verbal consent is obtained & procedure explained in detail. We need not stress that if male doctor should do the examination it will be in presence of a female nursing staff. During the examination findings of relevance are development of secondary sexual characters, presence or absence of galactorrhoea, signs of androgen excess like hirsuitism & thyroid enlargement. Sterile speculum examination is important to rule out vaginismus from other causes of dysparunia. This examination can also reveal any abnormality or discharge from the cervix. Bimanual examination gives idea about the size & mobility of uterus. Any abnormal finding in physical examination should be supported by laboratory & radiological evidences & should be treated before the treatment of infertility commences.
We start the clinical examination of female by measuring her weight & height & then calculating her BMI. Our experience has shown that ladies who have normal BMI not only respond well to the treatment of infertility but also have a better outcome of pregnancy as compared to their obese or underweight counterparts.
After recording the weight, the lady should be escorted into a comfortable examination room by a trained nursing staff where detailed general & systemic examination is done. Verbal consent is obtained & procedure explained in detail. We need not stress that if male doctor should do the examination it will be in presence of a female nursing staff. During the examination findings of relevance are development of secondary sexual characters ( breasts, axillary and pubic hair) , presence or absence of galactorrhoea, signs of androgen excess like abnormal hair growth & thyroid enlargement. Sterile speculum examination is important to examine cervix and vagina for any abnormality of signs of infection and to rule out vaginismus from other causes of dyspareunia. Bimanual examination gives idea about the size & mobility of uterus. Any abnormal finding in physical examination should be supported by laboratory & radiological evidences & should be treated before the treatment of infertility commences.
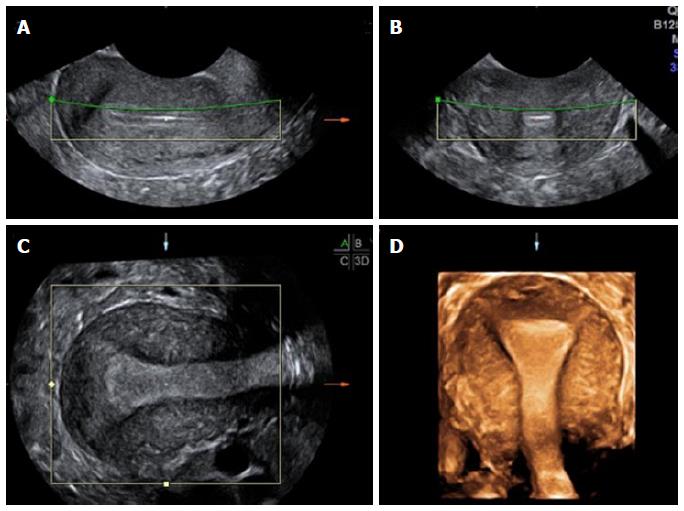
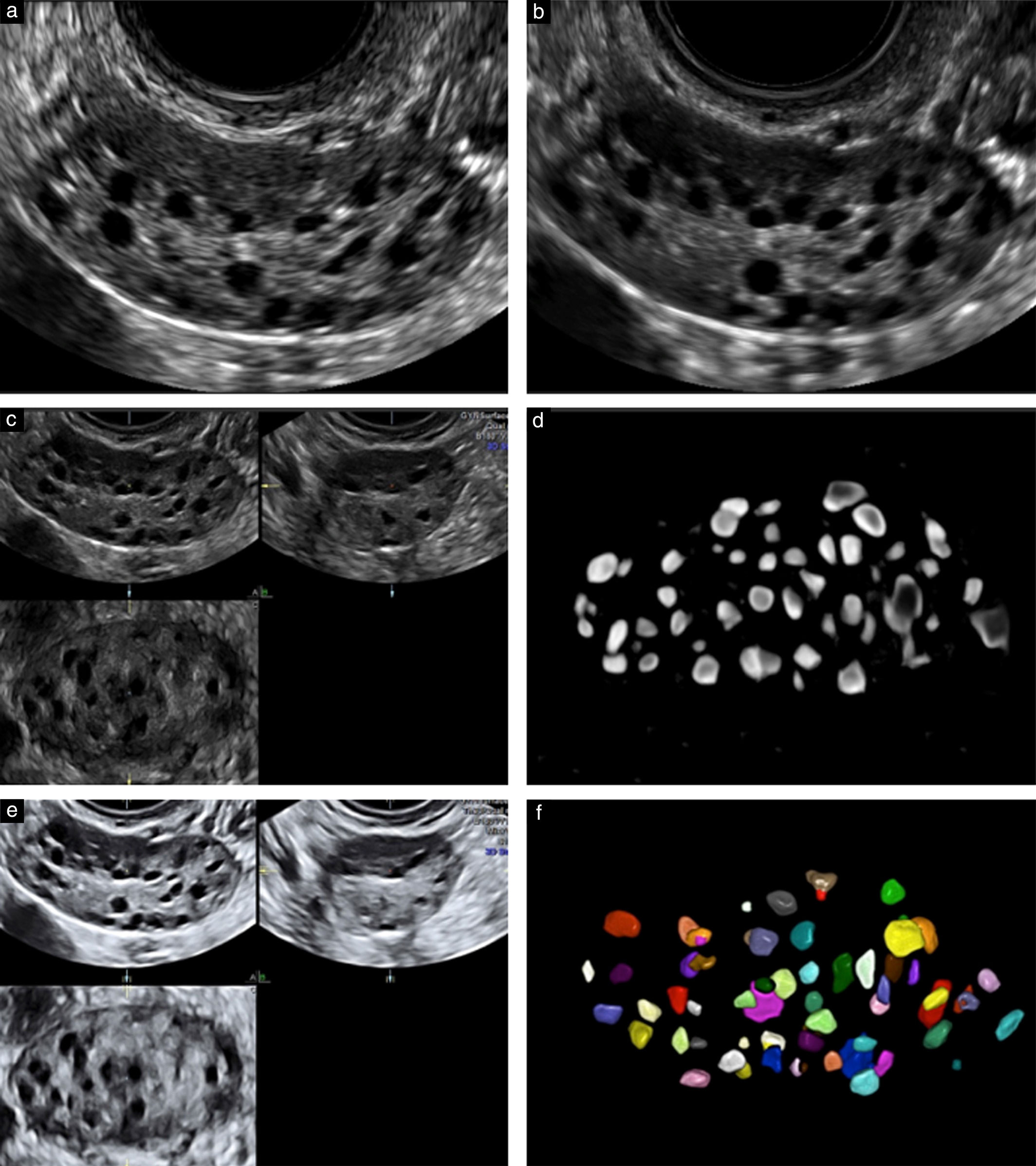
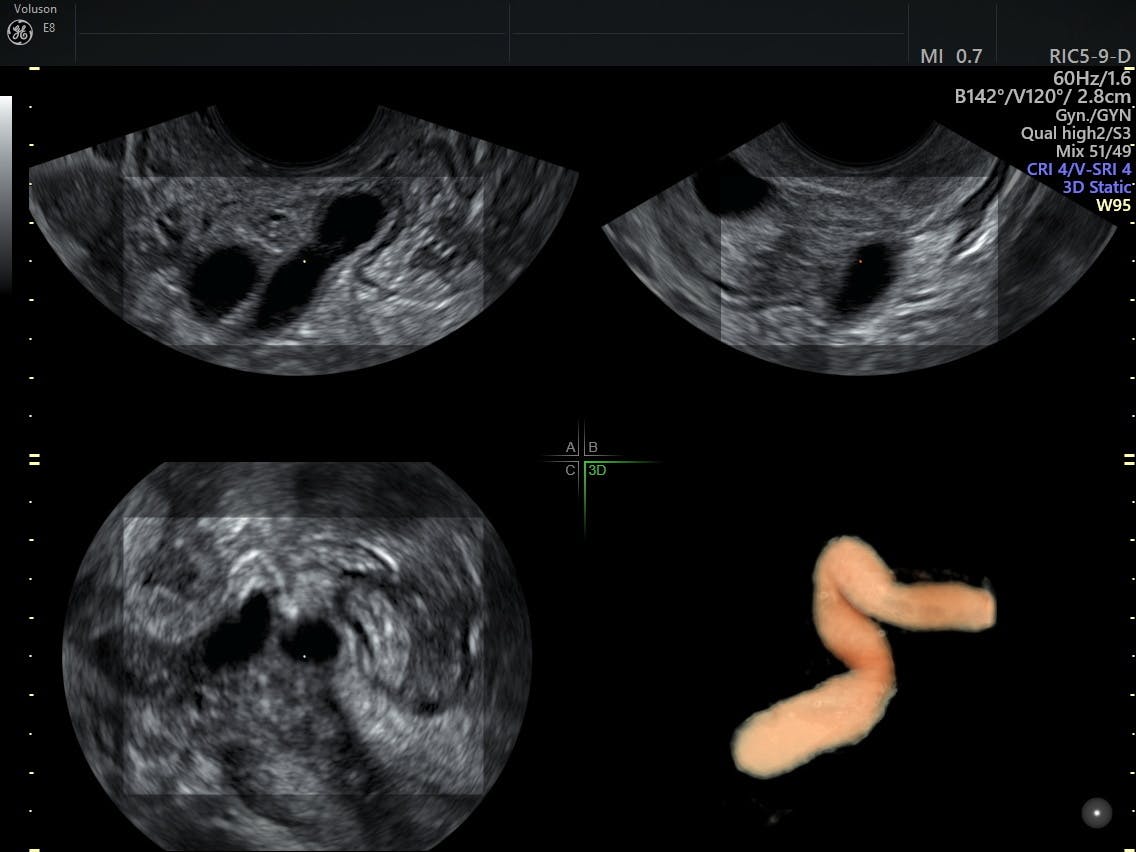
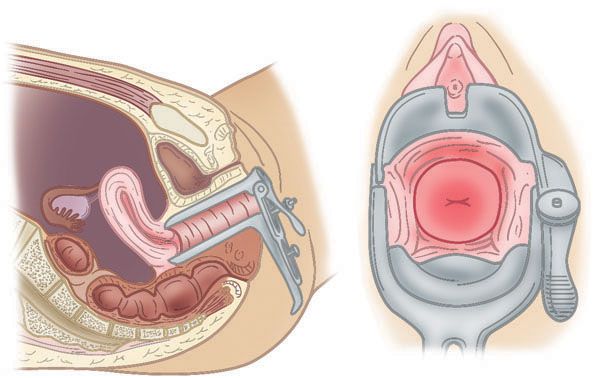
Trans vaginal sonography with 3D evaluation of uterine cavity has become the most important tool in the armamentarium of the physician to diagnose & treat infertility. TVS has a high sensitivity & specificity for follicular monitoring, prediction & conformation of ovulation.
While evaluating the female genital system by TVS, the examiner should scan every part in detail.
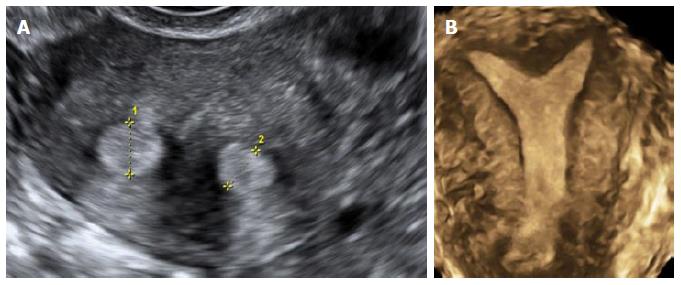
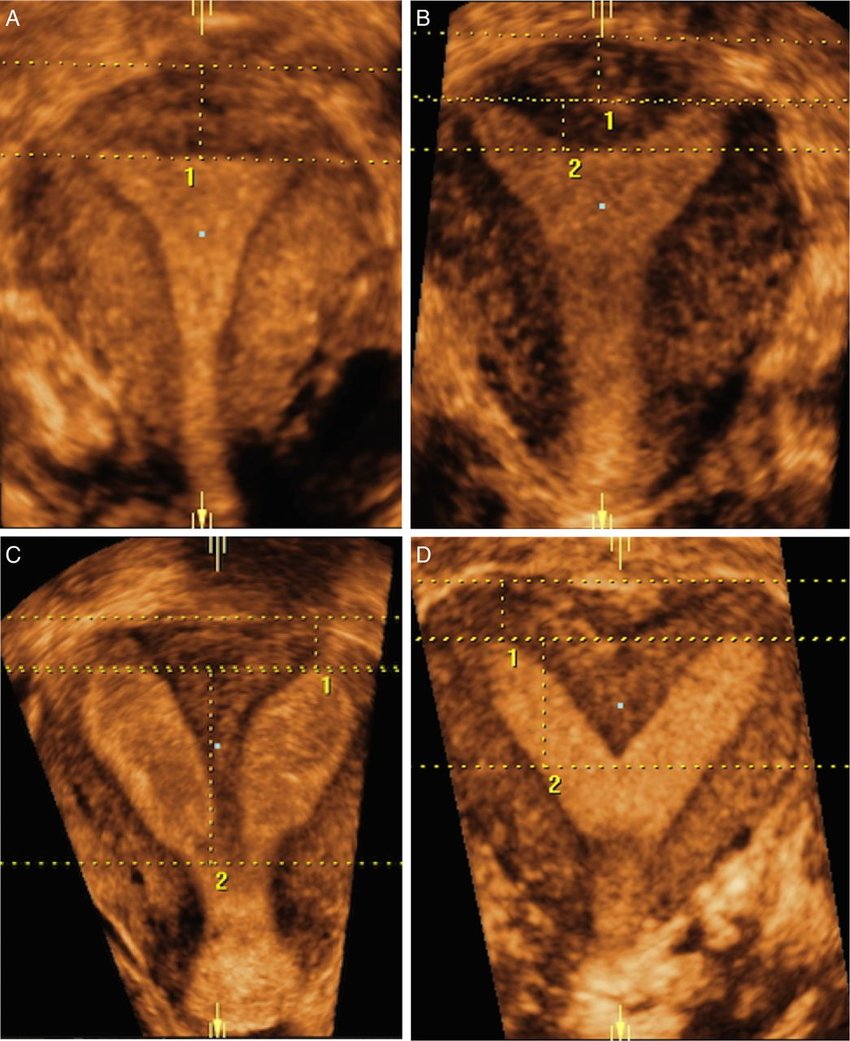
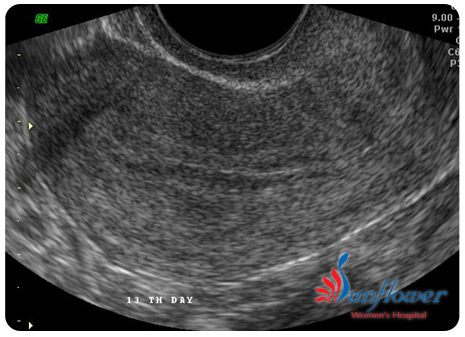
Trans vaginal ultrasound examination of the body of uterus is done to observe a detailed view of the myometrium & to diagnose any mullerian anomalies like septate uterus & bicornuate uterus , fibroid & adenomyosis.
Cervix is evaluated for the length of the cervix, nabothian cyst & cervical mucous.
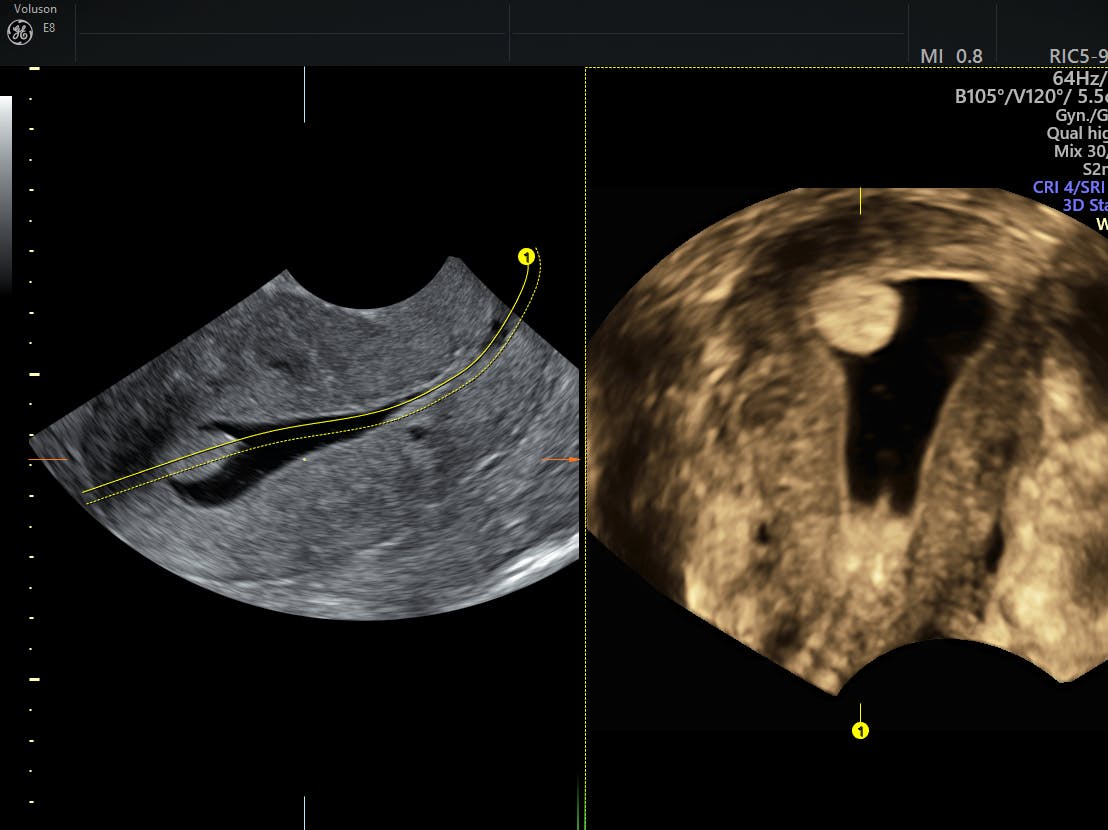
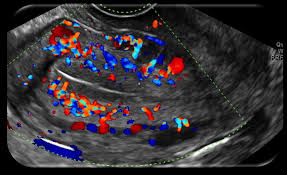
Endometrial cavity is scanned for endometrial thickness, endometrial pattern, endometrial polyps & presence of any foreign bodies or synechia, endometrial blood flow.
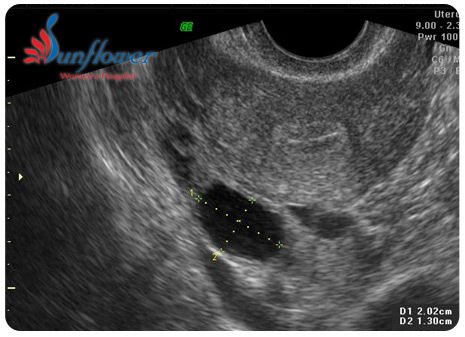
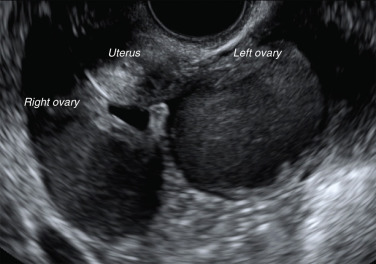
Apart from the location, mobility & size of the ovary, assessment of its volume & antral follicle count is also important to predict the outcome of any fertility therapy. Ovarian pathologies like functional cysts, PCO & endometriomas, tumors can be diagnosed by TVS.
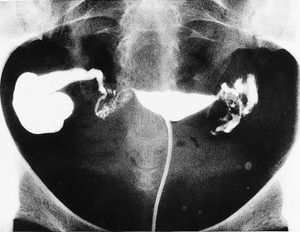
Healthy fallopian tubes are not visualized in a routine transvaginal scan (except if there is a massive fluid collection in the pelvis). Hence diagnosis of healthy tubes is a diagnosis of exclusion. But if fallopian tubes get infected and dilated (tuberculosis, pelvic inflammatory disease, endometriosis) i.e. hydrosalpinx they can be visualise on TVS.
Excluding the periovulatory period, any free fluid in pelvis should be tried to diagnosed & treated before commencement of any treatment.